Healthcare from the perspective of a clinician encompassing both the capture of the clinical viewpoint as well as the technology to help clinicians capture knowledge at the point of care
The thoughts expressed are my own and do not necessarily represent those of Nuance
The Panel "The Art of Medicine" Panel (part of the Art of Medicine campaign) took place yesterday from 9 - 11am at the Boston's W Hotel, 100 Stuart St, Boston, MA
Keith Dreyer, DO, PhD, FACR, Vice Chairman of Department of Radiology, Massachusetts General Hospital
Adam Landman, MD, MS, MIS, MHS, CMIO, Health Information and Integration at Brigham and Women's Hospital (@landmaad)
Steven J. Stack, MD, past chair of the American Medical Association (AMA); served on multiple federal advisory groups for ONC on HIT, practicing emergency physician
and at the far right moderated by Paul Weygandt, MD, JD, MPH, MBA, CCS, CPE, Vice President of Physician Services, Nuance Communications
And it was very well attended:
Today, physicians are struggling to serve their patients’ needs in a healthcare system that seems to work against them at every turn. While technology has the potential to vastly improve healthcare overall, issues remain when it comes to usability, data-entry and complementing patient care vs. competing with it.
In part 1 I have attempted to capture the underlying sentiments and thoughts form our panelists together with some thoughts on potential ways to help resolve these areas and problems.
The panel opened with the original Art of Medicine video:
The session was divided into several separate discussions - the first of which the Issues of today:
There has been an increasing burden placed on physicians to document more and more detail but no additional time to do this and in fact probably less and they struggle with the increasing information over load and the challenge of processing - As John Halamka put it:
"We need wisdom and today's #EHR make that hard to get from patient info to give me what I need now"
"3 petabytes of patient data...overwhelmed with data, we just need information, knowledge"
This is combined with the increasing regulations which the panel viewed as directly linked to the increasing need for HealthIT tools to help deal with these regulations. As Adam Landmaan put it the design of the EHR’s is based on the design focus and in the current fee for service health system is designed largely support the physicians to capture and document optimize for bill not for patient care
But I thought Keith Dreyer captured the sentiment well when he described technology as decreasing our ability to communicate
“I couldn't imagine dictating into a microphone in talking with my family "
And we are seeing declining capture off the patient’s story in the EHR
Some snapshots of ideas thoughts from our panelists included:
IT tools driving “note bloat” of information that is non-specific to the patient
Physicians need timely “wisdom” to positively effect patient care at the time of encounter
“Big bang” of government funding for EHR adoption has generated massive amounts of information that is, at present, unmanageable
At stage now of EHRs where they are “one size fits all,” so not customized to specific specialty/setting needs
Need to identify the smallest number of moving parts (IT tools) to facilitate patient care
Need for monolithic (“one size fits all”) IT solutions is driven by babel of nomenclature
Quality measures show that there is a problem, but not the causality
There was much more discussions and thoughts on solutions but one of the concepts that stood out for me was this one from Adam Landmaan straight out of the Television Reality show - copying the Shark Tank concept
That will be an interesting panel and team event and look forward to hearing the results
We need to return to the Art of Medicine and as one panelist put it:
People sought out Doctors in the past even when they actively hurt you and bled you
They did this because the doctor provided compassion and care that had the best intentions - they cared about their patient and the Art of Medicine
Physicians don’t act on business motives. They act on patient care motives.
You can see the #ArtofMedicine HashTag Social Media Statistics here and analytics here
Steven J. Stack, MD, past chair of the American Medical Association (AMA); served on multiple federal advisory groups for ONC on HIT, practicing emergency physician
Keith Dreyer, DO, PhD, FACR, Vice Chairman of Department of Radiology, Massachusetts General Hospital
Adam Landman, MD, MS, MIS, MHS, CMIO, Health Information and Integration at Brigham and Women's Hospital (@landmaad)
and moderated by Paul Weygandt, MD, JD, MPH, MBA, CCS, CPE, Vice President of
Physician Services, Nuance Communications
The panel is taking place this Thursday from 9 - 11am at the Boston's W Hotel, 100 Stuart St, Boston, MA. If you have not already you can register here: www.nuance.com/artofmedicine. The event is free of charge,
“If we want doctors to do better work, we need to give them better work to do.”
and to do that doctors have to engage in the design of these solutions and the clinical community and the #HealthIT world must address these issues:
Just as we can’t expect a patient with heart disease to know intrinsically to maintain a low-sodium diet, we can’t expect the healthcare industry to know how to fix everything unless we speak up and advocate for change (especially with the other loud voices of insurers and politicians speaking on “our behalf”)
Some solutions are not technical as this Tweet by "Dr K" @MedschoolAdvice)
Sitting down in room makes patients feel you've spent more time w/ them than if u stand whole time, even if u spent same time. So sit
— Dr. K (@medschooladvice) March 21, 2014
We have the rare opportunity to shape the future of healthcare infused with technology and I, for one, want to be part of developing a solution that helps the next generation of physicians offer that comforting touch as they deliver an even greater level of care to their patients
Download the Art of Medicine eGuide here and join me and the panelist on Thursday as they discuss they start to shape a better HealthIT future for everyone. I will be live tweeting from the panel (#ArtofMedicine) and will post a summary after the event.
I know I am biased as one of the lucky Google Glass Explorer as can be seen in this post from MedCity Watching for Wearables at #HIMSS14:
I think they are wrong and its not just Glass that will provide better more ready access to essential clinical data.
Not to say that the initial program like many launches have had their problems with early releases of technology not quite ready for prime time - remember the 1987 Apple Newton:
Mat Honan (one on the same “Epic Hack”) wrote a piece about his early experiences “My Year with Google Glass” that highlighted some early acceptance challenges
Glass is socially awkward
People get angry at Glass
Wearing Glass separates you
and I would add Glass interrupts normal conversations and social behavior - but that is all now and like the mobile phone I believe it will be come a natural part of our technical fabric. Think back to 2007 and how pulling out a phone in a meeting was frowned upon - now it seems part of the fabric of many of the meetings I attend.
But it was Mat’s commentary on the impact it had on his perception fo phones that really stuck out for me
Glass kind of made me hate my phone — or any phone. It made me realize how much they have captured our attention. Phones separate us from our lives in all sorts of ways. Here we are together, looking at little screens, interacting (at best) with people who aren’t here. Looking at our hands instead of each other. Documenting instead of experiencing.
From initial diagnosis through to surgical therapies, chemotherapy treatments and even end-of-life care, my job is to listen, assess and provide educated decisions that ultimately impact the health and wellness of another human being…. it’s my belief that when talking face-to-face with a patient about a care plan aimed at eradicating their body of a disease that threatens to take them away from their family, there’s no room for paper, computers and/or mobile devices. In these most intimate of conversations, the focus has always and must remain on the communication between the caregiver and the patient on the receiving end. That, in its purest essence, is what practicing the art of medicine is truly all about.
That’s not to say that Google Glass can solve this problem and in its current state and acceptance it might cause more challenges - but the potential is there to blend information access and capture into a physician patient interaction that remains all about the patient
Glass will provide improved access to essential clinical data to clinicians but as my friend Chuck Webster has pointed out on several occasions this is not just for clinicians. Patients are already accessing the internet in droves for clinical information, researching their conditions and that of their relatives and communities abound with resources and support for conditions from common to rare.
Before talking about some of the potential medical applications it is worth detailing the technology. Google Glass is basically a computer with 12Gb of memory attached to your head in the form of glasses. It has a heads up display with voice activation and has some apps that can be installed:
Facts
Google Glass is basically a computer attached to a pair of glasses
Google Glass has a display that is projected in front of the Right Eye that is a high resolution display equivalent of a 25 inch high definition screen from eight feet away
Google Glass has a camera that points forward and can take pictures (5MP) or video (720p) that is closely aligned with the view you see from your own eyes
Google Glass is voice activated using speech recognition to interact with the glass computer
Google Glass works best when connected to the internet
Google Glass Integrates with an Andorid Phone with a limited set of functions available for the iPhone
Google Glass has no built in illumination so pictures or video taken in dark conditions do not work well
The screen can be hard to see in bright light
There are many myths circulating:
Myths
If someone is wearing Google Glass they are recording me
False - The device is not set up to record continuously and will only record a video or photo based on an action by the wearer (either a spoken request
OK Glass, take a picture
or by pressing a button on the google glass device
Once Someone Has recorded something on Google Glass it is Publicly Posted
False - it requires an action on the part of the Glass owner to post the material to the internet otherwise it resides on the Google Glass device. It will be synchronized with the users Google+ account for automatic backup (much like photos are backed up from the iPhone to iCloud but like iCloud remain private to the user unless they elect to share them)
Google Glass is constantly capturing data and transmitting it to the Internet
False. Without an internet connection Google Glass simply stores any recorded information in the glass memory. And unless you have set it to record there is no data being captured
Google Glass tracks users and unsuspecting bystanders
False - Google Glass is not tracking or recording anything unless instructed to do so by the user
So who is using this technology, where are they using it and how are they using it in Healthcare. This article covered some of the early concepts and featured a short list of potential applications
Video sharing and storage: Physicians could record medical visits and store them for future reference or share the footage with other doctors.
A diagnostic reference: If Glass is integrated with an electronic medical record (EMR), it could provide a real-time feed of the patient’s vital signs.
A textbook alternative: Rather than referring to a medical textbook, physicians can perform a search on the fly with their Google Glass.
Emergency room/war zone care: As storied venture capitalist Marc Andreessen proposed in a recent interview, consider ”dealing with wounded patients and right there in their field of vision, if they’re trying to do any kind of procedure, they’ll have step-by-step instructions walking them through it.” In a trauma situation, doctors need to keep their hands free.
Helping medical students learn: As suggested by one blogger, a surgeon might live stream a live — and potentially rare — surgery to residents and students.
Preventing medical errors: With an electronic medical record integration, a nurse can scan the medication to confirm whether it’s the correct drug dose and right patient
In its simplest form just transmitting images in real time can offer some advantages for diagnosis - in Rhode Island they are planning on implementing Google Glass for the ED doctors to obtain real time consults with dermatologists.
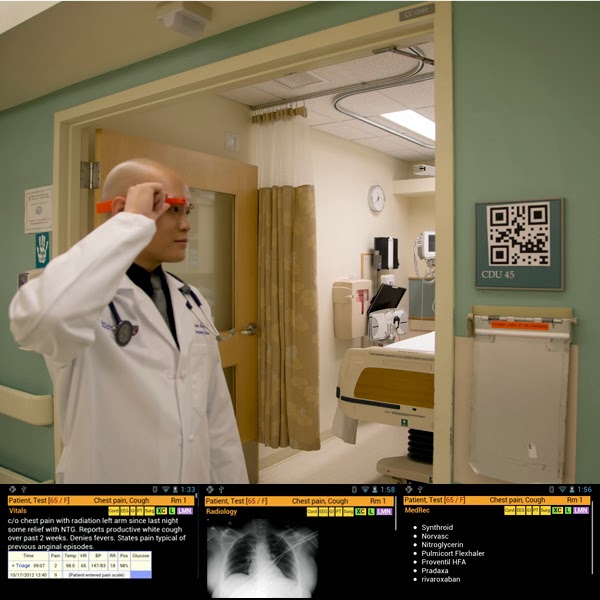
And this from Kareo showing a patient education application that records the physician patient interaction and then makes it available afterwards for additional review:
When a clinician walks into an emergency department room, he or she looks at [a] bar code (a QR or Quick Response code) placed on the wall. Google Glass immediately recognizes the room and then the ED Dashboard sends information about the patient in that room to the glasses, appearing in the clinician’s field of vision. The clinician can speak with the patient, examine the patient, and perform procedures while seeing problems, vital signs, lab results and other data.
And this concept by the way was top of everyone's wish list that I talked to in my unofficial survey of engaged and interested observers of my own pair. I'll paraphrase
If I could get it to recognize someone and provide me with their name when I meet them that would be fantastic!
But it is in urgent care where there is so much potential:
"If I want to look at for example radiology I can double tap ‘radiology...There's his chest x-ray, it just popped up, oh he's got a middle lobe pneumonia"
Part 2 will cover medical applications and how Google Glass technology can be applied in a busy clinical setting
The relationship between physicians and patients is at the core of healing. This begins with hearing and understanding. We want to reimagine healthcare—where physicians can get back to the art of medicine and were delighted to be joined by panelists:
Dr. Mark Kelemen, Senior Vice President, CMIO, University of Maryland Medical System Dr. Charles H. Bell, Vice President, Advanced Clinical Applications, Hospital Corporation of America (HCA)
Stuart James, CIO, Sutter Health Dr. Andrew Watson, CMIO, University of Pittsburgh Medical Center (UPMC) (@arwmd)
The panel was moderated by our very own
Dr. Paul Weygandt, Vice President, Physician Services, Nuance Keith Belton, Senior Director, Clinical Documentation Solutions Marketing, Nuance
and attended by some 50 attendees with varying backgrounds and perspectives
The underlying question:
How do return the focus to the patient. How can physicians navigate the changes and challenges of today’s complex healthcare environment while doing what matters most to them – listening and caring for patients?
The panel discussion addresses current physician frustrations with technology and what needs to change to keep them focused on patients and not data entry. It was clear that the physician’s voice and medical decision making is what matters most in practicing the art of medicine and how do physicians and patients both benefit?
We know from surveys that
36% of physicians say that EHRs interfere with face-to-face communication during patient care
80% of physicians say “patient relationships” are the most satisfying part of practicing medicine
28% of an average ER physician’s time is spent directly with patients
and from a recent HIMSS session interesting Patients prefer doctors to have an EHR
This is about the changing face of healthcare – it’s not just about technology. It’s about how we envision healthcare. How do we explain to providers that this isn’t about technology – this is about a new world order coming to healthcare
Posting every patients Magnesium level multiple times in a note is not good clinical care #artofmedicine #himss14
One of our panelists asked the audience:
How many Docs would go to facility with no #EMR and used paper - no hands went up
We do see value in Health Information Technology
One of the overriding concerns was the need for cultural change. The office or hospital based physician system is struggling to meet the patient needs today. They want to have the right nurse or physician there for them at the right time and indeed at the right place with telemedicine. It’s about cloud-based/consumer-based healthcare.
More consumer-friendly healthcare
We need to get back to that local physician practice – with technology in the middle as a supporting actor but not the main event
Technology cannot be an impediment to taking care of patients
Many physicians are in this field because we are trying to drive change but are struggling with the existing system that fail them. When I see a patient I have to review 10 systems, carry out at least 4 major systems examinations before I can submit a claim that properly reflects the care I delivered:
I am not taking care of the patient I am taking care of a computer
Dr Andrew Watson told the story of a patient under his care with a terrible antibiotic resistant infection that a patient developed in hospital and he was now under constant supervision adn intensive therapy. But as he said - he never needed to come into hospital - he could have been treated at home. Poignant reminder that Telemedicine is not just about reducing cost - it can be better for the patient and offer better results.
As a musician he remembers the implementation of the MIDI interface in the early 1980’s that allowed music manufacturers to create one standard that was royalty free and widely adopted for the benefit of the user musicians and the vendors. He wants that in healthcare - so do I.
Until we change the mandate on clinicians to document 8 of 10 systems to be fairly compensated for the care given
And importantly the concept of Bring Your Own Device (BYOD) is bringing functional tools into the healthcare setting and will/is revolutionize the care being delivered. As one panelist put it:
my iPad never complains, is always there, has the latest information and access to latest medical updates
To summarize:
We need strategies for bringing the focus back to the physician-patient interaction and removing impediments to that relationship
Healthcare organizations should be and are encouraging/valuing physician professionalism
This is about the changing face of healthcare – it’s not about technology. It’s about how we envision healthcare. How do we explain to providers that this isn’t about technology – this is about a new world order coming to healthcare
The Physician (#DrHIT) Symposium at #HIMSS14
Opening session was eloquently covered by Robert Wah, MD (@RobertWahMD) detailing the spectrum of issues ranging from the new Healthcare System:
The challenge of SGR “fix(es)” and the evolution of the systems we are implementing and the value proposition. As he put it
Quality of care is improved with better information — saving lives and money
As for Jonathan Teich and his session Improving Outcomes with CDS - he used his personal experience where peer pressure (as he described it 3rd time he was pressured to take on an expert triple diamond ski slope) he finally agreed and ended up in a serious ski accident fracturing multiple vertebrae. Interesting analogy relative to the Clinical Decision Support System and the pressure this applies to clinical practice sometimes inappropriately...
Interesting look at alerts and the potential for providing more than just alerts but actually providing intelligent data that distill down to 10 types of CDS interactions
Immediate Alerts: warnings and critiques
Event-driven alerts and reminders
Order Sets, Care Plans and Protocols
Parameter Guidance
Smart Documentation Forms Improving Outcomes with Clinical Decision Support: An Implementer’s Guide (HIMSS, Second edition, 2011)
Relevant Data Summaries (Single-patient)
Multi-patient Monitors and Dashboards
Predictive and Retrospective Analytics
Filtered Reference Information and Knowledge Resources
Expert Workup Advisors
And the important summary slide was the CDS Five Rights (Right information, people, formats, channels and times)
And returned to one of the core opportunities - Patient Engagement with a a session by Henry Feldman, MD FACP: Informatics Enabling Patient Transparency. He asked the same questions as another presenter - how many fo the audience considered themselves a patient (Still only a shabby 80%) and then took this further asking
You feel that you know exactly what your provider was thinking in making his decisions
You think the clinical systems helped your provider understand comprehensively everything about you
You build clinical systems or are a provider
With the inevitable decline in hands up
You think your (or anyone else’s) software truly helps the patient or even the provider understand comprehensively or transparently what is going on
Sadly we are not near this and the reality is much further with physicians thinking patients are unsophisticated. Yes at he pointed out the airline industry gets it and even the DMV/MVA gets it offering customer engagement models:
Their experience and stats blow the unfounded resistance out of the water
Only 2% of patients found notes more confusing than helpful
Only 2% found the note content offensive
92% said they take better care of themselves
87% were better prepared for visits
Importantly we need to turn data into information for patients and he cited the Wired example of a Laboratory test (Blood Test Gets a Makeover Steve Leckart) and the makeover for
Basic Labs
Cardiology Result
and the PSA result
I know where I'd like to be receiving my care (and lab results) from! Great finish to the session. So as he summarized where we should be with patient engagement an data
Open your data to your patients
Patients understand more than we think
Teach patients how to use data effectively – This can save you time in the long run
The new Art of Medicine campaign is focused on getting physicians back to their original roots - the reason we all stepped over the threshold of medical education and into an honorable profession to serve our community. Its all about the patient but changes in the healthcare system and in particular changes with technology have taken the focus away from our patients and onto the technology in our office. Recent study conducted by Northwester University highlighted the distraction physicians feel away form their patients by the EMR
As Steve Schiff, MD a practicing cardiologists puts it
As far back as I can remember, there was never a time when I didn’t want to be a physician. It’s a choice in which there is no equivocation: either you want to be a doctor or you don’t.
The campaign includes an e-Guide: The Art of Medicine in A Digital World replete with thoughts, suggestions and concepts to manage the digital world while remaining focused on the most important person in the examination room - the patient. The release was covered in this piece by HIT Consultant and referenced the panel taking place next month in Boston.
Many of the thoughts and ideas were captured in the Top 38 lessons from Digital Health CEO’s from Rock Health. I picked a few choice quotes that capture the spirit and intent fo the Art of Medicine for me:
“Healthcare is yet to be transformed by technology.” - Joshua Kushner “You need a degree of foolishness to cause disruptive change in healthcare. Dare to dream.” - Vinod Khosla “If you’re going to re-invent healthcare you have to start from scratch.” - Vinod Khosla “The key to good product is invisibility for the user.” “Partnership is going to be absolutely key to taking healthcare to the next transition in evolution.” - Sue Siegel
The campaign kicked off this week with this resource page - The Art of Medicine and a short video highlighting the challenges and opportunites
There will be much discussion at HIMSS14 around the topic and we are looking forward to hosting the panel on Thursday, March 27, 2014, 9:00-11:00 a.m. at Boston’s W Hotel. You can find out more and/or register here or come by our booth 3765 at HIMSS14.
“The science of medicine goes nowhere if you leave the human element out of the equation. Curing our patients starts with listening to them.”
During a recent and troubling discussion with a physician friend, he described to me a new ailment he’s been experiencing: waking up in the morning, and not looking forward to going to work. The reality is that he is not alone. It’s no secret that physicians across the country, regardless of their specialty or location, are reaching their limit for juggling new requirements, technology upgrades, and policy changes, all while trying to deliver personalized, quality care to their patients. As a result, busy physicians are, quite understandably feeling pressured and pulled away from direct patient care and critical clinical-decision making, and, at the end of the day, that is what matters most to patients and physicians alike.
It is easy to imagine the impact overloaded and dissatisfied physicians could have on Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores, and how these regulatory pressures and so many new healthcare technologies could be linked to the decline of the “art of medicine.” But are we, in fact, misdiagnosing the problem?
A recent study from Johns Hopkins University found that internal medicine interns are lacking proper bedside etiquette, which is not only essential to providing quality care, it directly impacts medical outcomes and patient satisfaction scores. Focusing on five key elements of proper patient-physician decorum, researchers tracked whether or not hospital interns:
Introduced themselves,
Explained their role in the patient’s care,
Touched the patient,
Asked open-ended questions, or
Sat down with the patient during the visit.
Results revealed that interns touched their patients (either during a physical exam, handshake or gentle, supportive touch) 65 percent of the time and asked open-ended questions 75 percent of the time, but introduced themselves only 40 percent of the time, explained their role merely 37 percent of the time, and actually sat down during only nine percent of the visits. Such results are disconcerting, at best, and reveal a more pressing truth: These basic and critical communication deficiencies that are essential to providing holistic patient care are not being taught.
The study exposes the reality that the shift away from patient focus and the “art of medicine” isn’t just stemming from increased physician workloads caused by new policies and changing technologies. It is infiltrating our profession through a change in training, as well. While we have reduced junior doctors’ work hours for safety reasons, we have not adjusted the overall length of training they receive. Medical students, our future physicians, are not receiving the holistic education that helps them balance keen scientific skills with compassionate delivery.
But, as they say, “knowledge is power,” and now that we are starting to pinpoint conditions that are tearing at our profession, we can start to heal them. We can’t expect our medical interns to know how to handle difficult and emotional situations unless we show them. We need to teach them how to engage with patients, earn their trust, really listen and understand them. They need to be able to view what their patients say through both a lens of science and medicine, as well as a lens of compassion and caring, in order to help them get and stay well.
And what of the technology challenges that are driving wedges between patients and physicians? While there is no denying that much of health information technology is putting pressure on physicians and forcing them to adapt to new methodologies, these challenges are a necessary to revolutionizing patient care. They are, in essence, the basis of growth and the very nature of science. If it weren’t for boldly trying new approaches, we might still be relying on leeches and blood-letting to cure melancholia. Just as we can’t expect a patient with heart disease to know intrinsically to maintain a low-sodium diet, we can’t expect the healthcare industry to know how to fix everything unless we speak up and advocate for change (especially with the other loud voices of insurers and politicians speaking on “our behalf”).
We must be mindful that as physicians, it is our sworn duty to defend the practice of delivering the best care to our patients from anything that threatens to impinge on that quality. We need to stay engaged and be responsive; and that also means we need to assist with diagnosing major technology pain points and identify when something isn’t working. We have the rare opportunity to shape the future of healthcare infused with technology and I, for one, want to be part of developing a solution that helps the next generation of physicians offer that comforting touch as they deliver an even greater level of care to their patients.
Many years ago I remember an excited friend who worked for one of the vendors of electronic medical records (really this was more of a billing and patient tracking and management system than and Electronic Health record) desperate to show me some of their new applications – in particular a module they had developed to capture clinical data. He pulled out his “laptop” (it was more of a luggable)
Fired up the application, selected a patient and proceeded to enter a blood pressure: click, click, click, click, click, click, click, click…..some 20 clicks later he had entered a blood pressure of 120/80. He was excited and I was not.
I am constantly reminded of this as I watch doctors interact with systems and especially with the ongoing focus on blood pressure (Did you know that May is the National High Blood Pressure Education Month) and the video challenge from ONC
“To create an under 2 minute compelling video sharing how they use health IT or consumer e-health tools to manage high blood pressure”
The winners can be seen here
Key to the challenge is having the data for monitoring as emphasized in the Six Sigma techniques of DMAIC
Define
Measure
Analyze
Improve
Control
Capturing that data without burdening our clinical staff who should be focused on the patient not on intrusive and distracting tasks of data entry. I made this point a number of years ago "Doctor Please Look at Me not Your EMR" that came from a personal experience in our local practice and as my then 10 year old succinctly put it at the time
“I wish the doctor had spent as much time with me as she did with her PC”
But data is essential and getting this into our medical record is essential to derive the value from these systems. So the study published in Journal of the American Medial Informatics Association (JAMIA): "Method of electronic health record documentation and quality of primary care" who’s conclusion implied that dictating clinical notes “appeared to have worse quality of care than physicians who used structured EHR documentation”.
Digging into the details suggested this was based on old data (2004 – 2008), measured the quality of documentation not the care and that choice in tools is the key to success in EHR implementations and clinicians satisfaction
There are good reasons that dictation as a means of capturing clinical documentation has been so successful for such a long time – it is easy to do, efficient and saves time. But the gap between the narrative text created and the clinical data we need to manage our patients widens with each report created. The JAMIA report highlighted the impact this can have on care, offering some insight into the potential decrease in the quality of care that results in disconnecting the clinician from the interaction and clinical decision support tools and data that is built into the EHR. But the process of entering this data must not intrude into the clinical interaction with patients. All is not lost – Natural Language Processing (NLP) tools are bridging this divide allowing clinicians to use their preferred method to capture the patient’s clinical information in narrative form and extracting out the discreet data that is essential for the EHR systems that need the data to drive the decision support tools and workflow processes.
So clinicians can have their cake and eat it too and best of all it allows them to return to the art of medicine and focus on the patient not the technology.
It can be frustrating to be a clinician in the era of the internet and instantaneous availability of data especially when the reliability and accuracy is variable. But this is the world we live in and there is plenty of data showing that patients are accessing information in ever increasing numbers. The challenge has been helping patients filter the data for both relevance and accuracy.
Vaccination has been at the epicenter of a these challenges for some years - in fact long before the wide spread use of the internet thanks to a piece published in The Lancet in 1998 and unusually retracted. In fact the BMJ published a paper in 2011 declaring the paper fraudulent - as they noted in the discussion the lead author (now stripped of his medical degree and academic credentials) was clearly actively perpetrating the fraud
Who perpetrated this fraud? There is no doubt that it was Wakefield. Is it possible that he was wrong, but not dishonest: that he was so incompetent that he was unable to fairly describe the project, or to report even one of the 12 children’s cases accurately? No. A great deal of thought and effort must have gone into drafting the paper to achieve the results he wanted: the discrepancies all led in one direction; misreporting was gross. Moreover, although the scale of the GMC’s 217 day hearing precluded additional charges focused directly on the fraud, the panel found him guilty of dishonesty concerning the study’s admissions criteria, its funding by the Legal Aid Board, and his statements about it afterwards
Sadly despite repeated studies and investigations. Despite the retraction of the original article by the Lancet. Despite the other authors personally retracting the paper we still hear about a “link”. Sadly some high profile individuals continue to perpetrate the fraud (notably the model Jenny McCarthy and most recently the “reporter” Katie Couric).
I saw the posting by Aaron Carroll MD, MS is a Professor of Pediatrics and Assistant Dean for Research Mentoring at Indiana University School of Medicine (the Incidental Economist) last week when he posted this map of the real effects of this in Vaccine Preventable Outbreaks (click on the map button on the left if necessary)
I was reminded of there Jerry Maguire movie clip when I read the latest in a long line of security breach stories - this one emanating from Canada where this group is in hot water over a massive 620,000 patient data breach…taking 4 months to notify authorities. Apparently Canada does not have a national Breach notification rule like the US and the public “Wall of Shame"
Canada does not have a federal health data breach notification requirement. But the Canadian provinces have their own rules, including some that mandate notification. Under Alberta's Health Information Act, which was enacted in 2001, the reporting of health data breaches is voluntary, privacy experts say.
They might want to change that...
In this latest release Medicentres Family Health Care Clinics, a 27-clinic medical group in Western Canada had an unencrypted clinic laptop stolen from one of the clinic's IT consultants.
The laptop contained 620,000 patient names, dates of birth, health card numbers, medical diagnoses and billing codes, officials said.
Here in the US the chart of complaints is depressing
How many more data breaches will we see before everyone understands the need to pay close attention to security.
Encrypting your hard drives for all machines that contain patient information and demanding all staff and consultants and anyone that has access to patient data encrypts their drive and data would have prevented this.
We know doctors are under an ever increasing load may eventually break their backs..if nothing else its increasing the overall pain
In a recent study of physician attitudes toward clinical documentation technology and processes clinicians the majority of clinicians said they would be more responsive to Clinical Documentation Improvement (CDI) clarifications if they were delivered in real-time within their normal documentation workflow in the electronic health record (EHR). They report being "disrupted" by queries for additional information
after they’ve documented in a patient chart or worse, after the patient is discharged. All believe that ICD-10 will make matters much worse
With #HealthIT a growing portion of how doctors do their jobs they want to be involved in technology decisions yet most were not involved in clinical documentation technology decisions for their organization. And timing is everything - going back to answer questions after you have left the patient or worse after the patient has left "the building".
So what is the difference between success and failure of a CDI program
As the study points out physicians’ growing dissatisfaction in being
saddled with processes that distract them from clinical care, while being excluded from the decision-making process of choosing things that impact them every day
Technology should be simple and work for physicians and the key to changing the experience is to eliminate rework
Rework in clinical documentation is the enemy of efficiency
As Brian Yeaman, MD CMIO for Norman Regional Health System puts it
Using things like CLU and applying that to the ICD-10 code book to help me refine that diagnosis or ask me whether it’s the left or right or an upper or lower extremity are tremendous because it has a significant impact on our bottom line, and it’s also a physician satisfier … and on the back side we are not getting so many coding queries
And Reid Conant, MD President and CEO of Conant and Associates says
“Now we can provide our physicians with tools to get real-time feedback to not only change that document, but also change their behavior for the next document. That’s what organizations are looking for, and frankly, that’s what the doctors are looking for.”
We can achieve ICD10 compliance without breaking the back of clinicians
This is not news for many in the healthcare profession as they face the challenges of billing rules and regulations and the sometimes obscure idiosyncrasy - but as you can see form this piece on NBC for many patients this is a surprise and a costly one at that
Hospitals are told that they "have to" use this status (Under Observation) if the patient doesn't meet a host of criteria for "Admission" all being driven by a series of guidelines that are publicly available although not well known and much of it in response to the RAC audits
All this is set to get worse with the “Two Midnight” rule (you can see some guidance here and some of the issues on this here)
Yes it does. Healthcare and in particular doctors are juggling far too many changes
And like the picture of Aaron Gregg who achieved the world record of the most catches of chainsaws in 2008 (88 btw) doctors are doing their best to keep up but they are reaching their limits. We continue to ask doctors to do more with less, their focus is forced further away from the physician-patient interaction.
Technology can help and Natural Language Processing is transforming how consumers interact with technology in a more conversational, natural way. And in Healthcare we have taken this approach and applied it calling it Clinical Language Understanding (CLU) and importantly will allow physicians to get back to the Art of Medicine
Amongst other things we can:
Simplify Interactions with the EHR
Balance the Need for Patient Narrative and Structured Data
Increase Documentation Specificity in Real-Time
Much like NLU has helped drive intelligent, natural interactions between consumers and technology, CLU will help re-humanize healthcare. By enabling physicians to focus on the patient, not the technology, providers can begin to embrace a next-generation approach to healthcare that will drive efficient, intelligent clinical decisions that impact each and every facet of patient care.
It’s an exciting time with CLU and NLP as a critical enabler in helping doctors be more productivity in the new digital era of healthcare and maintain focus on what matters most: patient care.
Declaration: I am a 23andMe customer - I liked the concept and was excited by the price point that made the service accessible and cost effective...so maybe that explains my quick reaction (per the Kübler-Ross model of grief of Denial, Anger, Bargaining, Depression, Acceptance) to many of the posts and negative feedback pushing back.
I am still processing the news and not sure exactly where I sit - personally I am glad I got in before the health information was blocked. Maybe this is a purely personal position coming from the privilege of being a physician. In fact this piece on Forbes/Quora: What Do Doctors Think About 23andme?
probably captures the viewpoint I have different from others. In fact the images summarize how many people might approach this
Hmmm - you can see the logic and while the point made that not all information is relevant or important my view is firmly on the side of the patient being allowed to make that decision themselves. It is always worrying to me that someone else is filtering information and making decisions as to what they consider to be important to me - how can they know?
The example cited is one of a fit healthy individual making a decision based on genetic testing that suggests they might be at increased risk of cardiac disease that needs to be put int he context of them being fit and healthy
In fact they state
This is why every ethical healthcare provider follows this mantra: do not order a test or perform a procedure if it will not change your management of the patient, because doing so may cause needless harm/risk to the patient and will cause needless damage to the patient’s finances.
A reasonable position and one perhaps we might expect the FDA to support.....yet the FDA allows for direct to consumer advertising in the US.....? That seems at odds with the stance taken on genetic testing. There is no doubting that extra testing can cause additional stress and concern - putting everyone into an MRI is a bad idea since we identify around 20% "findings" many (may even be most) of which are incidental. I personally am delighted with my 23andMe results that include genetic details and insights that help me make my own personal health decisions.
I gave up personal genetic information to 23andMe who like any other cooperation could misuse it, may not protect it sufficiently or may share it with insufficient privacy protections to shield me from being identified. But that was my choice and in this instance I felt the risks outweighed the benefits.
But the cynic in me can't help but think that this may all be money related especially given the recent spat over the BRCA gene testing that was recently struck down but remains the tip of the patent iceberg.
One worry is that people might undergo unnecessary tests and procedures based on the information 23andMe provides. For example, critics worry that a woman who is found to have a false-positive BRCA mutation might have a prophylactic mastectomy inappropriately. This seems to me to be an impractical concern. It is difficult imagine a surgeon operating in such a situation without first verifying the genetic testing through another lab and extensively discussing the benefits and risks of such an approach with the patient.
Quite - it might create a worthwhile discussion between a patient and their healthcare provider. In another example the risk of Alzheimer's which a customer might feel powerless to prevent but I would suggest that this may not be true in the future and as one friend and colleague told me when he shared his results that showed an increase risk of Alzheimer's:
It just means I am going to play more sudoku as I get older
That seemed like a good strategy and attitude. It is also important to note:
It turns out, however, that people seem to be less psychologically devastated by adverse genetic test results than many of the experts anticipated. For instance, a study published in the New England Journal of Medicine found that “in sample of subjects who completed follow-up after undergoing consumer genomewide testing, such testing did not result in any measurable short-term changes in psychological health, diet or exercise behavior, or use of screening tests.
On balance I'd rather have the choice than have the government make decisions about what data I can access. I say this with all due respect to my clinical colleagues who may disagree and the many that had exchanges with me in other social media forums.
I would also explicitly state that this is a personal view and does not represent that of my employer nor does it represent clinical guidance.
Nelson (Rolihlahla) Mandela or Mandiba as he was know to many
was an inspiration for many with his incredible strength and especially his compassion and moral courage despite his 25 year incarceration. His strength contributed to the Rainbow Nation. In the words of another early lost talent Bob Marley:
I Want you to know I'm a rainbow too
You can take the boy out fo Africa, but you can't take Africa out of the boy. Today I am proud to call myself an African and stand tall with the people of Africa at this time of sorrow
He managed to bring light into any situation and there are so many tributes across the web - you can read his biography here - hard to pick on any but I liked Richard Branson's here
and included this great version of the classic song by "Biko" that was performed by
Peter Gabriel performed Biko a cappella at the unveiling of Steve Biko’s statue and the whole crowd sang every word. He said: "I have been living with the words (of the song) for a long time. It is a sense of completion to be here." You could see tears in Madiba’s eyes - it was one of the most emotive moments of all of our lives.
The Nelson Mandela Foundation posted its own message. But it was his words that summed it up for me and I have quoted many times:
What counts in life is not the mere fact that we have lived. It is what difference we have made to the lives of others that will determine the significance of the life we lead.” — Nelson Mandela
My deepest sympathies and condolences to the Mandela Family, the Nation of South Africa, the Continent of Africa and his friends around the world
You can always rely on Hollywood to take concepts and extend them into the future - sometimes correctly (cloaking, holographic TV, forcefields and eco skeletons with mind control), sometimes incorrectly (aluminum dresses, atmosphere that is completely controlled, suspension bridge apartment housing). We have had speech recognition and Spock's request:
So it was no surprise to find the latest Hollywood idea is the "Her" - a lonely writer develops a relationship with a newly developed operation system
Intriguing and challenging our current concepts with an exploration of artificial intelligence, voice and natural language technologies. These new styled avatars understand, listen and decipher what we say and something that Nuance has been developing and reinventing the relationship that people and technology can have. We can engage with our devices on our own terms and we have show these concepts in healthcare with our very own Florence - who is getting ready to launch in 2014
Ambitious you say - maybe but imagine the environment with intelligent personal assistants that hear you, understand you, know your likes and preferences – and in our world exist across your doctors office, the phone, surgery, hospital and elderly care and hospice. Cool? Liberating? Impossible?
If you’re Nuance, the idea is not only brilliant – it’s our focus and drive as we reinvent the relationship between people and technology. It is the chance to connect with your devices on human terms and presents infinite possibilities for intuitive interfaces that adapt to you.
Liberating our clinicians to focus on the patient and providing patients with someone they can talk to, interact with and who does have time for them. That future - coming to a doctors office near you:
Dr. Elizabeth D. McKinley’s battled breast cancer for 17 years but this past spring discovered the cancer had spread to her liver, lungs and brain. Her choice was to undergo more treatment that would have potentially debilitating and mind altering effects on her or change course, accept death and work on getting the best out of what was left of her life...as she put it
..time with her husband, a radiologist, and their two college-age children, and another summer to soak her feet in the Atlantic Ocean...“a little more time being me and not being somebody else.”
And some of her fight was with her own family - the non-medical members
clinging to the promise of medicine as limitless
And the medical members of her family (her husband is a radiologist)
looking at her disease as doctors, who know the limits of medicine
Its not a difference in the effects of disease and death but rather an advantage of knowledge and information that lead to truly informed decisions "doctors have control over their quality of life before they die and this sadly is control that eludes most other members of society" and it would appear especially try here in the USA. More than half of deaths take place in hospital and not at home surrounded by people we love which is the way most say they want to "go".
So if you do nothing else this Thanksgiving - take the time to talk about the subject with the people you love and create and advance directive or living will. In many respects no better way to be thankful than to set out what is important and let everyone know, now when you are fit and healthy.
Wishing you all a very happy family and friend fill Thanksgiving
Its not that doctors don't want to die, its just that they knwo they know enough about modern medicine to know its limits, importantly they have talked about this with their families as they want to be sure that no heroic measures will be used during their last moments in this reality
And the chart demonstrating the big discrepancy between what doctors want in life saving measures vs the general public pretty much said it all
So this piece in the Atlantic took it a step further - tracing the history of CPR from the 1960 at Johns Hopkins where the surgeons had
...successfully resuscitated every one of the first 20 patients they treated, 14 of whom (70 percent) survived without brain damage or other ill effects
But their source patients were not typical (young and mostly healthy) and when you extrapolate that out to an elderly population survival can fall to as low as 0% a variation in the effectiveness when performed in the real world
But it was Hollywood adn the media that pushed these procedures into the general awareness suggesting
...that two-thirds of all (fictional) cardiac arrests portrayed on ER (and other doctor shows) involved young patients who had suffered rare events like drowning or lightning strikes, rather than old people with heart disease (who account for 90 percent of cardiac arrests in real-life settings.....most of these fictional TV patients did well, unlike the vast majority of CPR recipients in real life
Dr Peter Benton was well known as all in life saving heroics
In fairness Hollywood was dramatizing some real life events - and they applied their pixie dust to this as they have to many other things.
But the problem remains and health care professionals need to help their patients understand their disease and make good choices, bearing in mind that heroics and life saving may well be a significant driver as it was for Stephen Jay Gould who was diagnosed with a rare and deadly cancer with a median survival of eight months...but as he said in his essay "The Median Isn't the Message".
this median survival means that one-half of patients die within eight months but the other half live longer. Most important, because the mesothelioma survival curve has a very long “tail,” a few lucky patients will live a lot longer
In his case his experimental treatment may have contributed to his 20 year survival past the original diagnosis...leaving a legacy of hope.